The nursing profession is a Nobel one. Yes, more than doctors it’s the nurse who spends time with patients. They need to be medically sound to attend an emergency and give good care to patients. Having said this they work in hospitals for a stipulated time and handover their task to the nurse who takes the next shift. Therefore the communication between nurses about the patient is recorded and is called as a shift change report.
Coming to the actual point, this page will provide you with a free nursing shift change report sheet to download. Also, we have listed down some educative details about how to use the shift change report, what are the components present in it and the importance of this report. You can understand this information to effectively use the shift change report.
Hospitals, nursing homes, medical health care providers, and individual nurses can use this sheet for effective communication about the patient.
We can understand your concern and would like to clarify. SBAR (S – Situation, B – Background, A – Assessment, R – Recommendation) template and nursing shift change report sheets are not the same. Shift change report sheet will have the summary of the patient health progress and not the medical record as present in the SBAR template.
Enough of introduction and it’s time to get into the actual business.
Contents
What is the end of shift report and the elements included in the report template
As mentioned before, nurses work for 12 hours and change shift. They either work in the morning from 7 AM to 7 PM or in the evening from 7 PM to 7 AM the next day. This time varies from hospital to hospital it can be from 3 AM to 3 PM, 9 AM to 9 PM etc. However, there is a shift and of course, the nurse will leave hospital handing over the responsibility to the duty nurse. Unlike another profession, nursing job deals with people who are sick.
Therefore each nurse before leaving duty must update the nurse who takes charge for the next shift. Communicating about all patient information is not possible and appropriate too. Both nurses cannot remember all the details about different patients. So, we will use a report with details to be filled. This report is called the end of shift report. The duty nurse who takes over can read and start providing the care to the patients.
Importance of a nursing shift changing report sheet
- During duty, the nurse will attend many patients. Each one will have a different history, diagnosis, allergies to medicine, medicine, food etc. It is vital that the nurse make a note of that and pass on to the other nurse who takes duty. Whether or not medicine is given and other details to be informed to the doctor or patients relatives are noted down in the shift change report.
- It is a structured report which will help both the nurses who leave duty and takes charge to understand the patient condition at a glance.
- Giving information to the doctor will become easy and accurate details can be given by looking at the report.
- The workload for the nurse will be reduced as they need not remember each patient’s health condition but just refer to the sheet.
- Patients also will feel comfortable that their details are intact and there is no room for confusion. This will reduce their anxiety and can recover quickly.
- Overall giving the right treatment to the patient can be achieved with the help of this report.
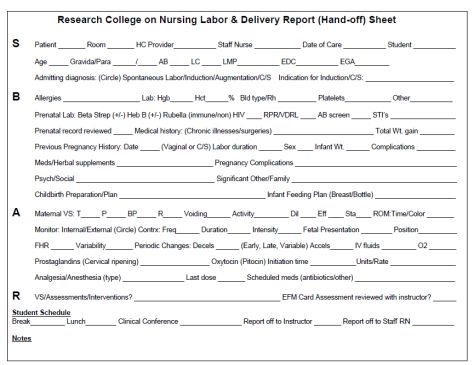
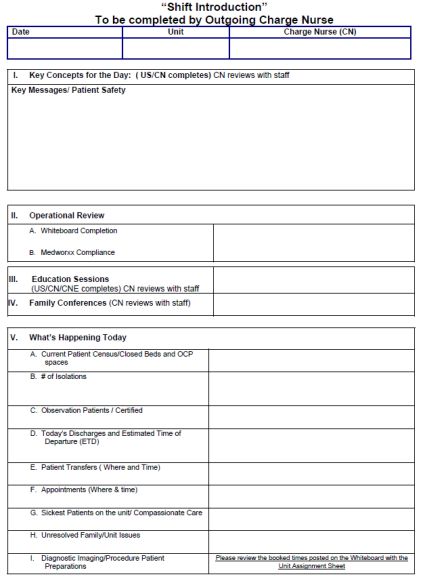
Structure & sample of nursing shift change report sheet
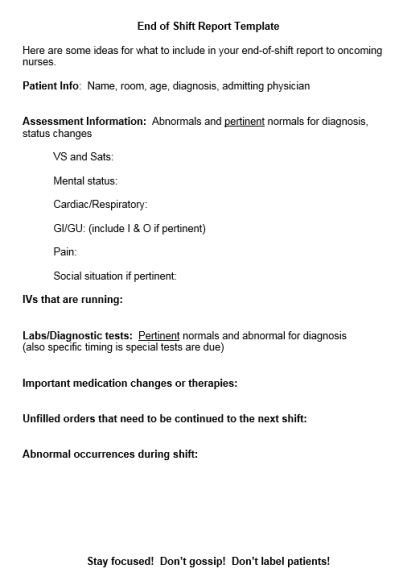
Image Courtesy – Registered Nurse RN
Now, let us walk you through the structure of a nursing shift change report sheet with samples. You can understand what all components are present, where they are placed and how to use them.
The different sections of the report include the
Patient Identification
Patient Name:___________________ Patient Room: _____________ DOB:___________ Sex:_____
Under the patient identification heading the patient’s name, id number given in the hospital, room number, age, gender, date of birth must be mentioned. Additional details like a patient’s father or spouse name and contact details also can be given in case if any emergency call needs to be placed by the nurse.
Doctor Details
Doctors:
Diagnosis:
Allergies:
History:
Here the name of the doctor who attends the patient and contact details must be given. Not all the doctor’s list but the one doctor who has referred the admission of the patient. For instance, a patient with an ortho problem will have one doctor who will treat. Others may be checking the patient for different reasons like surgery recommendation etc. But the primary doctor details to be presented for the nurse to reach out for any help at critical condition.

Patients History
Then the patient history, what was he/she admitted for. Do they have any complications in the past? What are they treated for and do they have an allergy to any drug or food etc must be recorded. The history will be one time input recorded at the time of admission. Diagnosis and allergy can be updated from time to time-based on any development in the patient’s condition.
Current Health Condition
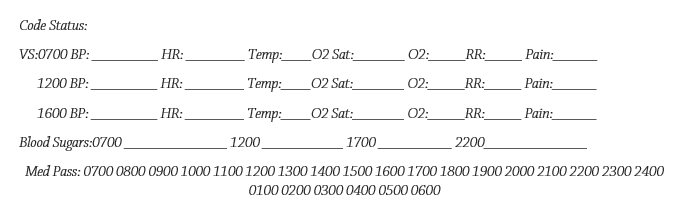
This section is important as the nurse must record the details monitored during their shift. The details can be the patient’s blood pressure, blood sugar, and other lab test done etc. Note: Edit this section based on your requirement and include details as desired.
Treatment Details
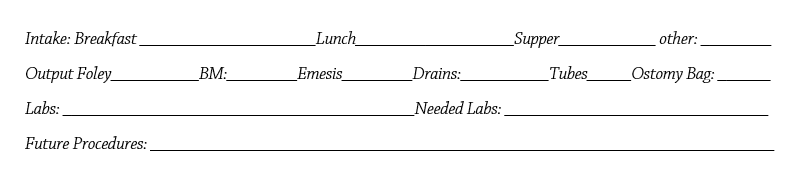
Next, comes the treatment details like what food is given and the future procedures. Again feel free to change this section with the specifics of the patient. Alternatively, design the sheet exhaustively as a one-time exercise and fill only places that are required.
Medicines
Note the medicines given. Change in medicine if any. Doctors might have visited and suggested some alteration in medicine dosage. All those needs to be recorded.
Food
Similar to medicine each patient will have a diet chart to be followed as recommended by the dietician and that needs to be updated for changes if any.
Recommendations
Finally include a section called comments, suggestions or recommendations. Name it the way you want to and here the nurse can write any inputs that they want to share with the other nurse.
Also, it is good to have a place for the nurse details so that they can fill their name and duty time which will help for any future reference.
How to do effective communication at the change of shift
Even though there is a sheet provided, education is required for each nurse in filling the report. So let us throw some light on how to fill the sheet for effective communication. Ok, we all understand that working as a nurse cannot happen per plan always. You may want to do something but land in doing something else. An emergency is an alarming word in nurse career. They may not find time to fill the sheet and finally put the patient’s life in soup. Yes, I am not criticizing, but the hard fact to digest. Several lives have become threatening due to lack of proper communication from the nurse during shift change. Follow these simple tips to improve communication and save a life.
Top 8 tips to improve communication 800x – For the kind attention of nurse’s
- Take time to read the report and fill in the sections. Do not fill for the sake of doing it. It is not a report that can have manipulated data. Never feel relaxed on the job and stay on the toe. One mistake will lead to blunder and you are dealing with human life.
- Once you read the report, then ask doubts to your seniors and then fill them. Have a practice of reviewing the report with the nurse on duty who is senior to you and get their opinion. Correct your language if required.
- Talk to the patients and understand them as well. Do not just go with the previous nurse report and manually fill the sheet.
- Record readings like temperature, BP, sugar etc soon after you test them on patients. Possible with time you record which will help give better treatment. Never procrastinate to fill report at the end as you will get confused with different patients or you may get into some other emergency later.
- Ask for the right medical terms to write your observation about the patient. Do not use generalized words which may not be interpreted well by the other nurse.
- Write neatly and let others read them without a problem. Take time to fill and if required highlight any important points to bring it to the doctor’s
- If you find any confusion, then ask and not simply fill the form.
- Try to check the patient’s basic details like name, age, etc before you continue to fill the form.
SBAR for shift change report
Yes, I agree that I mentioned shift change report and SBAR are two different reports. You may wonder why we talk about SBAR here. It is because in the latest studies carried out by Kean University nursing students they reported that SBAR way of communicating shift change will improve the overall communication.
Hence in this section, we will explain how you can use SBAR for shift change.
As already stated SBAR stands for situation, background, assessment, and recommendation. Find below how a nurse can communicate their message by splitting the change report into four sections.
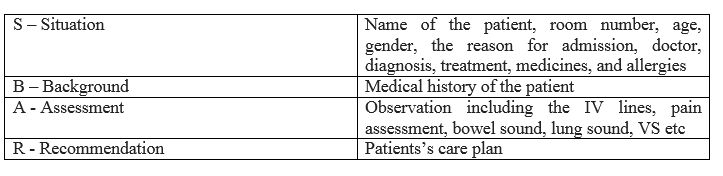
From the above illustration, you can understand the SBAR will help the nurse to mention details categorizing them and hence improves communication.
ICU Shift change report for nurses
We understand that nurses feel panic about attending ICU duty. Patients in the intensive care unit need extra attention and hence nurses must be vigilant all the time. So let us see how they can use the change report sheet for their best use.
First, understand that there is no need to panic but only need to be alert. So quickly get into the duty and check for the patient’s condition visually. Then go through the report given by the previous duty nurse. Attend the patient who needs immediate attention. Start filling the report then and there if you find the time. Else, at least have a sheet cheat to make a note of the bed number and updates. In ICU one may not find time to fill reports. The cheat sheet will help.
We strongly recommend using the shift change report as a bedside report so that all finer details can be marked instantaneously. Use the free sheets given here to you provide better care to patients in your hospital from today.
Also, we have uploaded sheets that require very less writing. Nurse in ICU might find it difficult to write stories. These templates have all details allowing the nurse to only enter the data like pressure, sugar, and all other observation values.
Key steps for a smooth nursing shift change
Reporting is the best way to have a smooth nursing shift change. Oral communication may not always help. One or two emergency cases can be reported orally to the oncoming nurse for providing immediate care. However, not all can be remembered. It is a good practice to use shift change sheet as an effective communication tool in between nurse.
Simple 5 step process to smooth the nursing shift change
Step#1 Have the report bedside of the patient and keep updating them. At the same time keep it out of reach of the patient. Let your details not panic them for many reasons.
Step#2 Stick to the point and no storytelling or beating around the bush while writing the report. Clearly, mention what is the status and what is expected from the oncoming nurse.
Step#3 Check with superiors for clarification and never be unsure about anything when you fill the report.
Step#4 Record the details on the sheet and not in your memory. Fill sheet soon after taking sugar or pressure test before you forget the value or confuse with the other patient.
Step#5 Arrive before so that you can observe things and get ready and can talk to the nurse on duty for inputs before you take charge.
Trust this will help. In case we missed something please do let us know to improve further and help nurse community to serve the society.